Community Health Promoters: Reimagining Comprehensive Care for Children With Sickle Cell Disease








Sickle cell disease (SCD) is a hemoglobinopathy that affects 500,000 newborns annually, the majority of whom live in sub-Saharan Africa.1,2 In Western Kenya, an estimated 20% to 25% of the population carries the sickle cell trait and approximately 1.5% of all infants born will have SCD.3,4 Due to lack of newborn screening, limited access to medications, and complications such as infection, it is estimated that more than half of children with SCD will die before age 5 in this setting.5-7 There is a critical need for equitable approaches to addressing this disparity.
In February 2023, Dr. Millicent Wanyama developed the first comprehensive SCD program in Bungoma County, Kenya. As the only pediatrician at Webuye County Hospital in Bungoma, she had been caring for children with severe complications of undiagnosed or untreated SCD — infection, acute chest syndrome, pain crises, splenic sequestration, stroke — and knew there was an unmet need. Even with the weekly clinic, she believed that care should extend beyond the hospital to the rural communities where her patients lived.
In August 2023, we proposed to partner with community health promoters (CHPs) in two sub-counties of Bungoma. CHPs are community members who bridge the gap between communities and health facilities. They are selected through a community-based process and receive a small stipend for their service. The CHP model originated in the mid-20th century to improve access to care in medically isolated regions. CHPs often have longstanding rapport with their communities, living in the regions where they are working. They know the language, culture, and customs, as well as the unique challenges that their communities are experiencing. Globally, their role has been valuable in promoting health, preventing the spread of disease, and providing basic therapies, while referring more complex cases.8-10
In partnership with Dr. Wanyama and Webuye County Hospital, we received the American Academy of Pediatrics Health Equity Grant to conduct a training of 260 CHPs within Webuye East and Webuye West (Figure). The first day focused on addressing misconceptions, genetics, clinical features, and management, as well as clarifying referral pathways. On the second day, CHPs participated in case scenarios to identify children with suspected SCD, counsel caregivers, and link families to care. Each CHP received a brochure with a summary of SCD and a referral form for use in the community.
Since partnering with CHPs, we have seen numerous ways their involvement has benefited children with SCD and their families. We have continued to see clinic attendance grow (Table), evidenced by an increase in newly enrolled patients. Families report greater awareness and decreasing stigma in their communities. CHPs have become crucial partners in tracing children lost to follow-up and emphasizing the importance of early care. The training has strengthened the bridge between hospital and community, empowering CHPs to advocate independently.
At the same time, we continue to experience barriers, namely financial constraints, that limit CHPs. Many CHPs lack resources, such as cellular airtime, to easily reach families or contact health facilities for medical guidance. Similarly, financial constraints often prevent families identified at the community level from accessing hospital services. These barriers highlight the urgent need for additional funding to strengthen referral systems, provide CHPs with essential support, and reduce financial obstacles for families. Without sustained investment in these interventions, the gains achieved risk being limited to this pilot effort.
In June 2024, Dr. Wanyama received the Fogarty LAUNCH Fellowship from the National Institutes of Health’s Fogarty International Center to initiate newborn screening for SCD in Bungoma. Already, CHPs are playing a fundamental role in informing communities about newborn screening and tracing mothers whose infants with SCD are lost to follow-up. The CHPs demonstrate the power of linking hospital-based expertise with community-driven care. With sustained support, these efforts can be scaled to transform outcomes for children with SCD, reduce preventable deaths, and foster healthier futures.
Figure. How community health promoters function in the care pathway for children with sickle cell disease
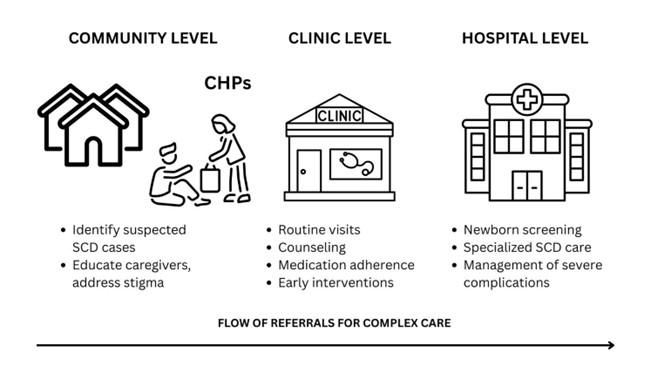
Abbreviations: CHPs, community health promoters; SCD, sickle cell disease.
Table. Summary of sickle cell disease comprehensive care program outcomes in Bungoma County, Kenya, as of January 2024
| Program Metric | Number |
| CHPs trained | 260 |
| Children enrolled in SCD care | 291 |
| New SCD diagnoses | 20 |
| Average clinic visits per patient (SD) | 1.6 (0.9) |
| Female : male ratio | 151 : 140 |
| Families with SHIF | 35.4% (n=103) |
| Families paying out of pocket | 63.6% (n-185) |
| Catchment area population | ~250,000 |
Abbreviations: CHPs, community health promoters; SCD, sickle cell disease; SD, standard deviation; SHIF, Social Health Insurance Fund (previously National Health Insurance Fund).
- Piel FB, Patil AP, Howes RE, et al. Global epidemiology of sickle haemoglobin in neonates: a contemporary geostatistical model-based map and population estimates. Lancet. 2013;381(9861):142-151.
- Quarmyne M-O, Bock F, Lakshmanan S, et al. Newborn screening for sickle cell disease and thalassemia. JAMA Health Forum. 2025;6(3):e250064.
- Mutua B, Sowayi G, Okoth P. Distribution of hemoglobinopathy phenotypes in western Kenya: a retrospective study done at Aga Khan Hospital, Kisumu. Egyptian J Intern Med. 2022;34(1):50.
- Aluoch JR. Higher resistance to Plasmodium falciparum infection in patients with homozygous sickle cell disease in western Kenya. Trop Med Int Health. 1997;2(6):568-571.
- Williams TN. Sickle cell disease in sub-Saharan Africa. Hematol Oncol Clin North Am. 2016;30(2):343-358.
- Green NS, Zapfel A, Nnodu OE, et al. The Consortium on Newborn Screening in Africa for sickle cell disease: study rationale and methodology. Blood Adv. 2022;6(24):6187-6197.
- Mano RM, Kuona P, Misihairabgwi JM. Determination of birth prevalence of sickle cell disease using point of care test HemotypeSC™ at Rundu Hospital, Namibia. BMC Pediatr. 2024;24(1):323.
- Perry HB, Zulliger R, Rogers MM. Community health workers in low-, middle-, and high-income countries: an overview of their history, recent evolution, and current effectiveness. Annu Rev Public Health. 2014;35:399-421.
- Ignoffo S, Gu S, Ellyin A, et al. A review of community health worker integration in health departments. J Community Health. 2024;49(2):366-376.
- Kwemoi KC. The role of community health workers in bridging gaps in access to care. Eurasian Exp J Sci Appl Res. 2024;6(3):1-7.
Disclosure Statement: The authors indicated no relevant conflicts of interest.
Acknowledgment: This article was edited by Ryan Mack, PhD, and Andrew Volk, PhD.