Case Study: 44-Year-Old Man with Fever, Abdominal Pain, and Pancytopenia
A 44-year-old man presents with fever, abdominal pain, and fatigue. His physical examination shows splenomegaly. His laboratory results are as follows:
| White blood cells | 2.0 K/μL (4.0-11.0 K/μL) |
| Hemoglobin | 7.6 g/dL (13.5-17.5 g/dL) |
| Platelets | 65 K/μL (150-400 K/μL) |
| Aspartate aminotransferase | 634 U/L (11-47 U/L) |
| Alanine aminotransferase | 164 U/L (7-53 U/L) |
| Alkaline phosphatase | 221 U/L (38-126 U/L) |
| Total bilirubin | 4.6 mg/dL (0.3-11 mg/dL) |
| Direct bilirubin | 3.1 mg/dL (0-0.3 mg/dL) |
| Fibrinogen | 100 mg/dL (170-400 mg/dL) |
| Ferritin | 123,000 ng/mL (22-322 ng/mL) |
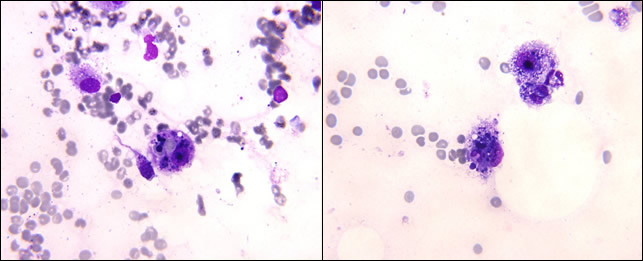
The patient is transfused several units of packed red blood cells without significant correction of his anemia, and instead, his pancytopenia worsens. Peripheral smear shows pancytopenia without blasts, tear drop cells, or dysplasia. A bone marrow biopsy demonstrates the following:
| Figure1 | Figure2 |
 |
|
- Aplastic anemia
- Acute promyelocytic leukemia
- Myelofibrosis
- Hemophagocytic lymphohistiocytosis
- Myelodysplastic syndrome
Answer
- Hemophagocytic lymphohistiocytosis
Explanation
The most likely diagnosis is hemophagocytic lymphohistiocytosis (HLH). The patient fulfills at least five of the main nine diagnostic criteria of HLH including fever, splenomegaly, cytopenia, elevated ferritin, low fibrinogen, and evidence of hemophagcytosis on bone marrow, as demonstrated in the pictures that a histiocytes engulfing a nucleated red cell (Figure 1) and a neutrophil (Figure 2).
Myelofibrosis can be associated with splenomegaly, but is less likely here since no marrow fibrosis or tear drop cells reported. Myelodysplastic syndrome is a possible cause of pancytopenia, but no dysplasia was noted on peripheral smear or in the bone marrow. Acute promyelocytic leukemia can be associated with DIC and low fibrinogen on presentation, but should have a hypercellular bone marrow with predominance of promyelocytes. Patients with aplastic anemia are found to have profound hypocellular bone marrow, but no hemophagocytes should be found.
Case study submitted by Tzu-Fei Wang, MD, The Ohio State University, Columbus, OH