COVID-19 Takes a Toll on People with Blood Cancers and Disorders
Studies aim to evaluate impact of COVID-19-related infection, treatments, and vaccination across this uniquely vulnerable population
(WASHINGTON, Dec. 11, 2021) – As the COVID-19 pandemic continues to evolve, five studies being presented during the 63rd American Society of Hematology (ASH) Annual Meeting and Exposition shed light on the persisting burden that COVID-19 has had on people with underlying blood disorders.
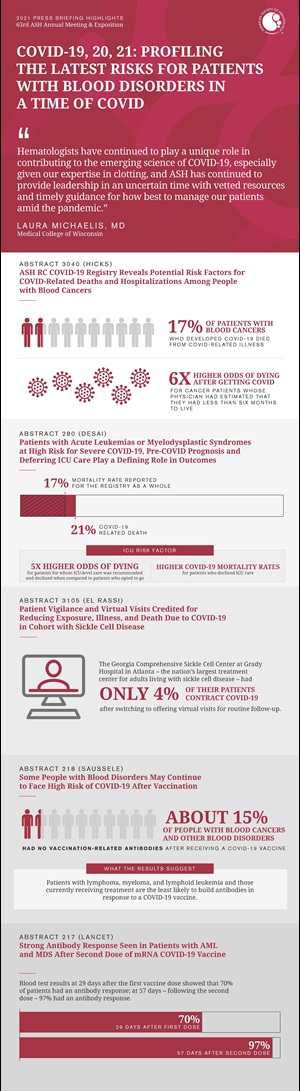
“We take care of the patients at the highest risk for COVID-19 illness and those who are among the least likely to respond to the vaccine; these and other studies underscore the dual vulnerability facing many of our patients,” said press briefing moderator, Laura Michaelis, MD, of the Medical College of Wisconsin. “Hematologists have continued to play a unique role in contributing to the emerging science of COVID-19, especially given our expertise in clotting, and ASH has continued to provide leadership in an uncertain time with vetted resources and timely guidance for how best to manage our patients amid the pandemic.”
Two studies analyze data from the ASH Research Collaborative (ASH RC) COVID-19 Registry for Hematology, which started in the early days of the pandemic to provide real-time observational data summaries to clinicians on the front lines of the fight against COVID-19, as well as researchers and providers around the world. In September 2021, the Centers for Disease Control and Prevention (CDC) awarded the ASH RC funding to identify the overall burden of COVID-19, the effects of health disparities and outcomes, and the areas where future resources should be focused for treatment for people living with hematologic malignancies. Specifically, CDC funding, in part, supports additional data submissions to the ASH RC COVID-19 Registry, real-time public data summaries, and research activities. As the Registry dataset has grown, researchers have identified potential drivers of severe illness, hospitalization, and mortality. The data also suggest that aggressive supportive treatment of COVID-19 can improve outcomes for many patients and should be offered.
A third study conducted among individuals living with sickle cell disease (SCD), suggests COVID-19 infection can cause occlusive events, resulting in pain episodes, but these patients seem to respond to COVID-19 treatments and also were quick to adopt precautions and shift to virtual appointments as needed.
The final two studies look at antibody response following vaccination among people with various hematologic malignancies, helping give clues into which groups of patients may still be at high risk of COVID-19 after getting the vaccines.
“A number of studies have shown that people with blood cancers have less than optimal responses to vaccination, and there is a need to continue to push for mitigation strategies,” said Dr. Michaelis.
This press briefing will take place on Saturday, December 11, at 12:30 p.m. Eastern time in press briefing room A315.
ASH RC COVID-19 Registry Reveals Potential Risk Factors for COVID-Related Deaths and Hospitalizations Among People with Blood Cancers
3040: Risks for Hospitalization and Death Among Patients with Blood Disorders from the ASH RC COVID-19 Registry for Hematology
Patients with blood cancers, particularly those with more advanced disease, are especially vulnerable to serious COVID-19 outcomes, including an elevated chance of severe illness and death from COVID-19, according to an analysis of more than 1,000 patients in the ASH RC COVID-19 Registry for Hematology. Based on the report, 17% of patients with blood cancers who developed COVID-19 died from COVID-related illness, a strikingly higher mortality rate than what was seen in the general population, according to researchers. Older age, male sex, poor cancer prognosis, and electing to defer intensive care when it was recommended were all independently associated with a heightened chance of dying.
“In our analysis, having a poor prognosis for underlying disease prior to COVID-19 and deciding to forgo ICU-level care for that disease were the most powerful predictors of mortality among patients with blood cancer and COVID-19–and the two may very well be related,” said Lisa K. Hicks, MD, MSc, of St. Michael’s Hospital in Toronto, Canada. “If someone is sick enough to require ICU-level care and their preference is not to receive this type of care, we would expect that decision to have a major impact on their survival.”
According to the data, patients whose physician had estimated that they had less than six months to live due to their cancer before getting COVID-19 had six-fold higher odds of dying and these odds nearly doubled among people who decided to forgo more intensive care due to COVID-19. However, these groups represented a small proportion of the overall sample with only 7% estimated to have a pre-COVID-19 prognosis of under six months, and 9% deferring ICU care.
Of particular interest to the field was whether blood cancer treatment would affect COVID-19 mortality. Most patients included in the dataset (71%) received cancer treatment during the previous year; others were either in remission or had not yet needed treatment. In addition, receiving cancer treatment in the year prior to COVID-19 infection did not significantly increase the risk of death as some had feared; however, it was linked to an increased risk of hospitalization if infected by COVID-19. Older age, being male, having active cancer, and having other health conditions were also associated with an increased risk of hospitalization from COVID-19 among patients with blood cancers.
“In the early days of the pandemic, there was a lot of uncertainty about whether we should withhold or modify blood cancer treatments in regions with high levels of COVID-19,” said Dr. Hicks. “The data are somewhat reassuring in that, while recent cancer treatment was linked to a higher risk of hospitalization among those with blood cancer and COVID-19, it wasn’t independently associated with a statistically greater likelihood of dying. The type of blood cancer was also not associated with a higher risk of COVID-19 mortality. These findings suggest that patients who need treatment for their hematologic malignancy should likely proceed with that treatment.”
Data were collected between April 1, 2020, and July 2, 2021, as part of the ASH RC’s COVID-19 Registry for Hematology, which is a public-facing, volunteer registry reporting outcomes of COVID-19 infection in patients with underlying blood disorders. A total of 1,029 patients from around the globe were included in this analysis. Of these, 41% were female. The median age was 50-59 years of age, and patients ranged from five to more than 90 years of age; 27% had at least one co-existing condition such as heart disease, hypertension, respiratory disease, or diabetes. Researchers sought to identify factors associated with a higher likelihood of hospitalization and death from COVID-19.
Of people included in the analysis, 354 (34%) had acute leukemia or myelodysplastic syndromes (MDS), 255 (25%) had lymphoma, 206 (20%) had plasma cell dyscrasia (myeloma/amyloid/POEMS), 116 (11%) had chronic lymphocytic leukemia (CLL), and 98 (10%) had myeloproliferative neoplasm (MPN). Patients with MPN and plasma cell dyscrasia had less severe COVID-19 illness overall compared to patients with CLL, leukemia, MDS, or lymphoma, which Dr. Hicks said is not surprising as patients with MPN typically live with their disease for many years, are generally in better health, and may not require immunosuppressive treatment.
“The data from the ASH RC COVID-19 Registry has limitations and findings should generally be regarded as hypothesis generating,” Dr. Hicks said. “Nonetheless, the data do suggest that patients with blood cancers are at substantial risk from COVID-19; this finding has implications for our patients, how we manage our clinics amid COVID-19 and the changing variants, and how vaccines, boosters, and antibody treatments are distributed.”
In this analysis, 17% of those with blood cancers died of COVID-19; the mortality rate among those infected with SARS-CoV-2 in the general U.S. population has been reported to be between 1.6 and 6.2% at various times during the pandemic, Dr. Hicks added.
The ASH RC Registry is a public voluntary registry that continues to accrue cases and provide the information on a public dashboard to help keep the hematology community apprised on changing trends. Dr. Hicks said the team will also be looking at how the risks of hospitalization and death changed as vaccines and COVID-19 treatments became more widely available.
Lisa Hicks, MD, MSc, will present this study during a poster presentation on Saturday, December 11, at 5:30 p.m. Eastern time in Hall B5.
Patients with Acute Leukemias or Myelodysplastic Syndromes at High Risk for Severe COVID-19; Pre-COVID Prognosis and Deferring ICU Care Play a Defining Role in Outcomes
280: Clinical Predictors of Outcome in Adult Patients with Acute Leukemias and Myelodysplastic Syndrome and COVID-19 Infection: Report from the American Society of Hematology Research Collaborative (ASH RC) Data Hub
In separate analyses of 257 patients with acute leukemia or MDS who developed COVID-19 and are part of the ASH RC COVID-19 Registry for Hematology, both neutropenia (a type of low white blood cell count) and having active MDS or leukemia (versus being in remission) were found to strongly and independently predict severe COVID-19 illness. Once hospitalized, active disease by itself – whether someone was newly diagnosed or had relapsed – was not tied to a greater odds of dying from COVID-19, nor was receiving ongoing cancer treatment.
For this retrospective analysis, which included data from 135 patients with acute myeloid leukemia (AML), 82 with acute lymphocytic leukemia (ALL) and 40 with MDS who were diagnosed with COVID-19 from 2019 to present, researchers sought to identify characteristics that put patients at higher risk of severe illness or death from COVID-19. At the time of COVID-19 diagnosis, 46% were in remission and 44% had active disease. COVID-19 severity was defined as mild (no hospitalization required), moderate (hospitalization required), or severe (ICU admission required). After adjusting for several risk factors, active disease and neutropenia at the time of COVID-19 diagnosis were also associated with severe COVID-19 illness that necessitated ICU-level care.
Overall, one out of five (21%) patients died from COVID-19, which was higher than the mortality rate reported for the registry as a whole (17%) or what was seen in the general public during the same period of time, researchers reported. Mortality among hospitalized patients with COVID-related illness was 34%, and mortality among patients once admitted in the ICU was 68%. The two factors most strongly associated with a higher likelihood of dying among these patients were: 1) how long someone was perceived to live from the underlying MDS or leukemia before getting COVID-19, as defined as a physician’s estimated prognosis of less than six months survival, and 2) whether or not they decided to go to the ICU if it was recommended. Older age, male sex, and neutropenia at diagnosis were also associated with COVID-19 mortality though less strongly.
“This is a particularly vulnerable population and we suspected they may do worse because they are immunocompromised and, as it is, the average survival for acute blood cancers if untreated is three to six months, so if COVID-19 comes together with that diagnosis, it’s very concerning,” said Pinkal Desai, MD, MPH, of Weill Cornell Medical College, New York. “Our data suggest these patients can survive COVID-19 and their underlying disease itself was not associated with worse mortality, which means that if these patients are given appropriate and aggressive treatment, we can help them recover. But if there are decisions that are made after they get to the hospital (for example, whether to go to the ICU) that clearly plays a role.”
In fact, patients for whom ICU-level care was recommended and declined had five times higher odds of dying compared with patients who opted to go to the ICU.
“Patients who went to the ICU did better regardless of disease status,” said Dr. Desai. “Just having acute leukemia or MDS puts these patients at high risk of severe COVID-19, and they need to be hospitalized and receive treatments, but decisions about the ICU should be individualized, a patient’s prognosis should be discussed, and if a patient wants aggressive care for COVID-19 that should be offered.”
Patients were more likely to forgo ICU care if they were older, male, smokers, or if they had active disease or an estimated pre-COVID-19 survival of less than six months. Forgoing ICU care was associated with a higher COVID-19 mortality in all patients.
“Our data show that these patients do survive COVID-19 after receiving care in the ICU and underscore that cancer treatments should not be withheld as inferior treatment would quickly put many of these patients into the category of a prognosis of less than six months,” said Dr. Desai. “COVID-19 vaccination is also critically important.”
The data are limited in that they were collected before COVID-19 vaccines were widely available; future data should inform about mortality rates among vaccinated patients.
Pinkal Desai, MD, MPH, will present this study during an oral presentation on Saturday, December 11 at 2:00 p.m. Eastern time in B312-B314.
Patient Vigilance and Virtual Visits Credited for Reducing Exposure, Illness, and Death Due to COVID-19 in Cohort with Sickle Cell Disease
3105: COVID-19 Infection and Outcomes at a Comprehensive Sickle Cell Center
The Georgia Comprehensive Sickle Cell Center at Grady Hospital in Atlanta – the nation’s largest treatment center for adults living with sickle cell disease (SCD) – quickly switched to offering virtual visits for routine follow-up care of its more than 1,300 patients as the COVID-19 pandemic emerged. People living with SCD, an inherited disorder characterized by crescent- or sickle-shaped red blood cells, are immunocompromised and thus at high risk for COVID-19. The center established a database to track all COVID-19 cases among its patients.
The first report from that database – the largest single-center study to date on COVID-19 in people with SCD – now shows that between March 2020 and March 2021, just 55 (4%) of the center’s 1,343 patients contracted COVID-19, of whom 16 (29%) were hospitalized and two ultimately died from complications of infection with the virus. Eleven patients (20%) required neither hospitalization nor emergency-room treatment for complications of either COVID-19 or SCD during the one-year follow-up period.
“Our findings show that when supported by virtual visits, most of our patients successfully reduced their exposure to and complications from COVID-19,” said study author Fuad El Rassi, MD, of Emory University and director of research at the Grady Comprehensive Sickle Cell Center. “They understood the risks and followed recommendations to stay at home and avoid interacting with other people.”
The 55 patients who contracted COVID-19 were aged 28 on average and 51% were female. Of those who visited an emergency room or were hospitalized during the year of follow-up, 27 (49%) sought care for a painful episode of SCD and 15 (27%) for complications of COVID-19. Among those who sought care for COVID-19 symptoms, 32 (58%) had pain as their primary symptom, followed by cough and fever (40%) and shortness of breath (31%); 25% had chest x-ray evidence of pneumonia. Sixteen patients received treatment, with nine receiving the antibody treatment remdesivir, eight receiving the steroid drug dexamethasone, and seven receiving red-blood-cell products to treat pain.
Twenty cases of COVID-19 were diagnosed between March and September of 2020. The two patient deaths from COVID-19 occurred in June and July of 2020. Among the 35 cases diagnosed between October 2020 and March 2021, no patients died and the number of hospitalizations decreased as better treatments for COVID-19 became available.
One of the patient deaths was due to a blood clot in the lungs, Dr. El Rassi said. “This unfortunately occurred before it became the standard of care to treat hospitalized COVID-19 patients with blood thinners,” he said.
“Despite the second peak in COVID-19 cases in the winter of 2021, there were no reported deaths among our patients who developed the disease,” Dr. El Rassi added. “This suggests that the patients’ vigilance in staying home may have been crucial to reducing illness and death, and having the option for virtual visits was also key.” Patients who needed blood tests or to obtain medication refills were sent to satellite centers.
Patient adherence to COVID-19 precautions was measured based on their responses to physician questions at intake and during virtual follow-up visits.
Dr. El Rassi and his colleagues plan to conduct further studies to evaluate the impact of the delta variant on diagnosis, illness, and death from COVID-19 among the sickle cell center’s patients.
Fuad El Rassi, MD, will present this study in an oral presentation on Monday, December 13, at 6:00 p.m. Eastern time in Hall B5.
Some People with Blood Disorders May Continue to Face High Risk of COVID-19 After Vaccination
218: Antibody Response to Vaccination with BNT162b2, mRNA-1273, and ChADOx1 in Patients with Myeloid and Lymphoid Neoplasms
According to a new study, about 15% of people with blood cancers and other blood disorders had no vaccination-related antibodies after receiving a COVID-19 vaccine. While researchers say it is encouraging that 85% of study participants did show an antibody response, the findings suggest that additional precautions may be warranted to prevent COVID-19 infection among people with blood disorders.
The study examined antibody levels after COVID-19 vaccination in people with blood cancers such as lymphoid and myeloid neoplasms, autoimmune disorders, and non-cancerous disorders of blood or immune cells. The results suggest that patients with lymphoma and those currently receiving treatment are the least likely to build antibodies in response to a COVID-19 vaccine.
“Some patients with hematologic diseases do not have an adequate antibody response and might, therefore, not have sufficient protection from vaccination,” said Susanne Saussele, MD, of III. Medizinische Klinik, Medizinische Fakultät Mannheim, Universität Heidelberg, Germany. “This study can help guide vaccination strategies for these patients. In addition, our study suggests that when it is possible to delay beginning treatment for their underlying disorder, it may be best to wait so that a patient can receive a vaccine or booster first.”
People with blood disorders face a high risk of hospitalization and death if they become infected with COVID-19, especially if they are older or have received therapies that reduce B-cells, a type of immune cell. Since the majority of participants in the study did respond to COVID-19 vaccines, the results underscore the role of vaccination as an important strategy for preventing severe disease, researchers said. However, the findings also suggest vaccination should be complemented with other precautions. “We should recommend ongoing protective measures such as masks, social distancing, and screenings, as well as prioritizing vaccination for family members and caregivers to protect the patients,” Dr. Saussele said.
For the study, the researchers recruited 373 patients treated for blood disorders at University hospital Mannheim in Germany and measured vaccine-related antibodies in their blood a median of 12 weeks after final vaccination. More than 90% of participants had blood cancer, while 9% had either autoimmune disease or a non-malignant blood disorder. Most patients had received the Pfizer/BioNTech vaccine; 10% received the Moderna vaccine, 7% received the AstraZeneca vaccine, and 6% received one dose from each of the two vaccine types.
Overall, 85% of participants tested positive for vaccine-related antibodies and 15% tested negative. The rate of negative antibody results was highest among those with lymphoid neoplasms, a group of diseases that include lymphoma, myeloma, and lymphoid leukemia. Among these patients, 36% tested negative for vaccine-related antibodies. Patients with indolent non-Hodgkin lymphoma, a slow-growing type of lymphoma, had the weakest response to vaccination overall.
Being on active therapy was associated with a reduced antibody response. Overall, 61% of study participants were on active therapy. Of those who tested negative for vaccine-related antibodies, most (71%) were on active therapy. Therapies correlated with a negative response were rituximab, ibrutinib/acalabrutinib, and ruxolitinib.
“Our study suggests that most people with blood malignancies – not only those who are currently under treatment – should monitor their antibody levels and work closely with their care team to determine how to continue to protect themselves from COVID-19,” Dr. Saussele said. “Antibody measurements offer a hint of who has responded to the vaccine and can perhaps ease up on precautions a bit.”
Dr. Saussele noted that the results are limited in that the study did not examine participants’ T-cell response to vaccination, meaning that some patients’ level of protection may have been underestimated. The researchers plan to continue to measure antibody levels for at least a year and to assess participants’ rates of breakthrough infections and response to vaccine boosters.
Jil Rotterdam, MD, Medizinische Klinik, Medizinische Fakultät Mannheim, Universität Heidelberg, will present this study in an oral presentation on Saturday, December 11, at 2:00 p.m. Eastern time in Hall B308-B309.
Strong Antibody Response Seen in Patients with AML and MDS After Second Dose of mRNA COVID-19 Vaccine
217: Responses to SARS-Cov-2 Vaccines in Patients with Myelodysplastic Syndrome and Acute Myeloid Leukemia
In one of the largest studies to date of the antibody response to vaccination against COVID-19 in people who had been treated for acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS), patients responded well to two doses of the Moderna mRNA vaccine and saw a particularly dramatic increase in levels of antibodies against the virus after receiving their second vaccine dose.
“We observed a strong antibody response to the vaccine in a group of patients at high risk for severe COVID-19, including among patients who were on active treatment for AML or MDS,” said Jeffrey Lancet, MD, of the H. Lee Moffitt Cancer Center and Research Institute in Florida. “The fact that antibody levels increased so dramatically after the second vaccine dose suggests potential utility in additional dosing, even for patients who initially respond poorly to the vaccine.”
Previous studies had shown that patients with other types of blood cancer – specifically, B-cell lymphomas or chronic lymphocytic leukemia – often have a poor antibody response to vaccination with one of the COVID-19 mRNA vaccines. Treatment of these cancers suppresses the ability of the immune system to produce white blood cells such as B cells and T cells to fight off infection.
“The treatment of myeloid cancers such as AML and MDS, including allogeneic transplantation, also suppresses white blood cells and leaves patients vulnerable to infection,” said Dr. Lancet. “We conducted this study to find out whether patients with these cancers would also have a suppressed or absent immune response to COVID-19 vaccination.”
The study involved 46 patients who either had previously or were currently undergoing treatment for AML or MDS. The patients’ median age was 68 years; 59% were male and 96% were white. On average, they were about two years out from the diagnosis of their cancer. Fifteen patients (33%) were receiving treatment for their cancer at the time they were vaccinated. Thirty-two patients (70%) had undergone a transplant of blood-forming stem cells from a healthy donor as part of their cancer treatment. Forty patients (87%) were in remission when they were vaccinated. (Note that some patients are counted twice – e.g., if they had undergone a stem cell transplant and were in remission, they would be counted in both categories. For this reason, the percentages add up to more than 100%.)
All patients received a first dose of the Moderna mRNA vaccine (this vaccine type was being given at the clinic) in late January 2021 and a second dose four weeks later. The investigators collected blood specimens from each patient before each vaccine dose was administered and again at four weeks after the second dose. The primary aims of the study were to describe the immune response and assess the safety profile of the vaccine in a cohort of patients with AML or MDS.
Blood test results at 29 days after the first vaccine dose showed that 70% of patients had an antibody response; at 57 days – following the second dose – 97% had an antibody response. Antibody levels were significantly higher after the second dose compared with after the first dose. Patients’ antibody response was not significantly affected by age, gender, race, disease status (i.e., active or in remission), time from disease diagnosis to vaccination, number of treatments patients had undergone for their cancer, whether patients had received a stem cell transplant, or whether they were on active treatment at the time of vaccination.
The most common adverse events following vaccination were the typical ones reported after vaccination with a COVID-19 mRNA vaccine, such as fatigue, headache, arm swelling, and mild pain at the injection site.
“The study results should be confirmed in a larger group of patients,” Dr. Lancet said. “However, based on these data, we feel comfortable advising patients with AML or MDS that they should get vaccinated against COVID-19. Due to their vulnerability to COVID-19, they stand to benefit from the vaccine more than most.”
This is an observational study without an identified control, or comparator, group, Dr. Lancet cautioned. Another limitation is that because the participants were overwhelmingly white, it is not known whether patients of other races or ethnicities would show a similar antibody response. In addition, the actual protective effect of the vaccine and the T-cell responses to it in this patient population are not yet known; the researchers are currently gathering these data.
The investigators are now following the same cohort of patients to determine whether a third dose of the vaccine can achieve even higher antibody levels than were seen after the second dose.
Akriti Jain, MD, Moffitt Cancer Center, will present this study in an oral presentation on Saturday, December 11, at 2:00 p.m. Eastern time in Hall B308-B309.
Additional press briefings will take place throughout the meeting on immunotherapy, new insights into blood disorders, diversifying care in acute leukemia, and selected late-breaking abstracts. For the complete annual meeting program and abstracts, visit www.hematology.org/annual-meeting. Follow ASH and #ASH21 on Twitter, Instagram, LinkedIn, and Facebook for the most up-to-date information about the 2021 ASH Annual Meeting.
The American Society of Hematology (ASH) (www.hematology.org) is the world’s largest professional society of hematologists dedicated to furthering the understanding, diagnosis, treatment, and prevention of disorders affecting the blood. For more than 60 years, the Society has led the development of hematology as a discipline by promoting research, patient care, education, training, and advocacy in hematology. ASH publishes Blood (www.bloodjournal.org), the most cited peer-reviewed publication in the field, and Blood Advances (www.bloodadvances.org), an online, peer-reviewed open-access journal.
Contact:
Leah Enser, American Society of Hematology
[email protected], 202-552-4927