Duffy-null Associated Neutrophil Count (DANC)
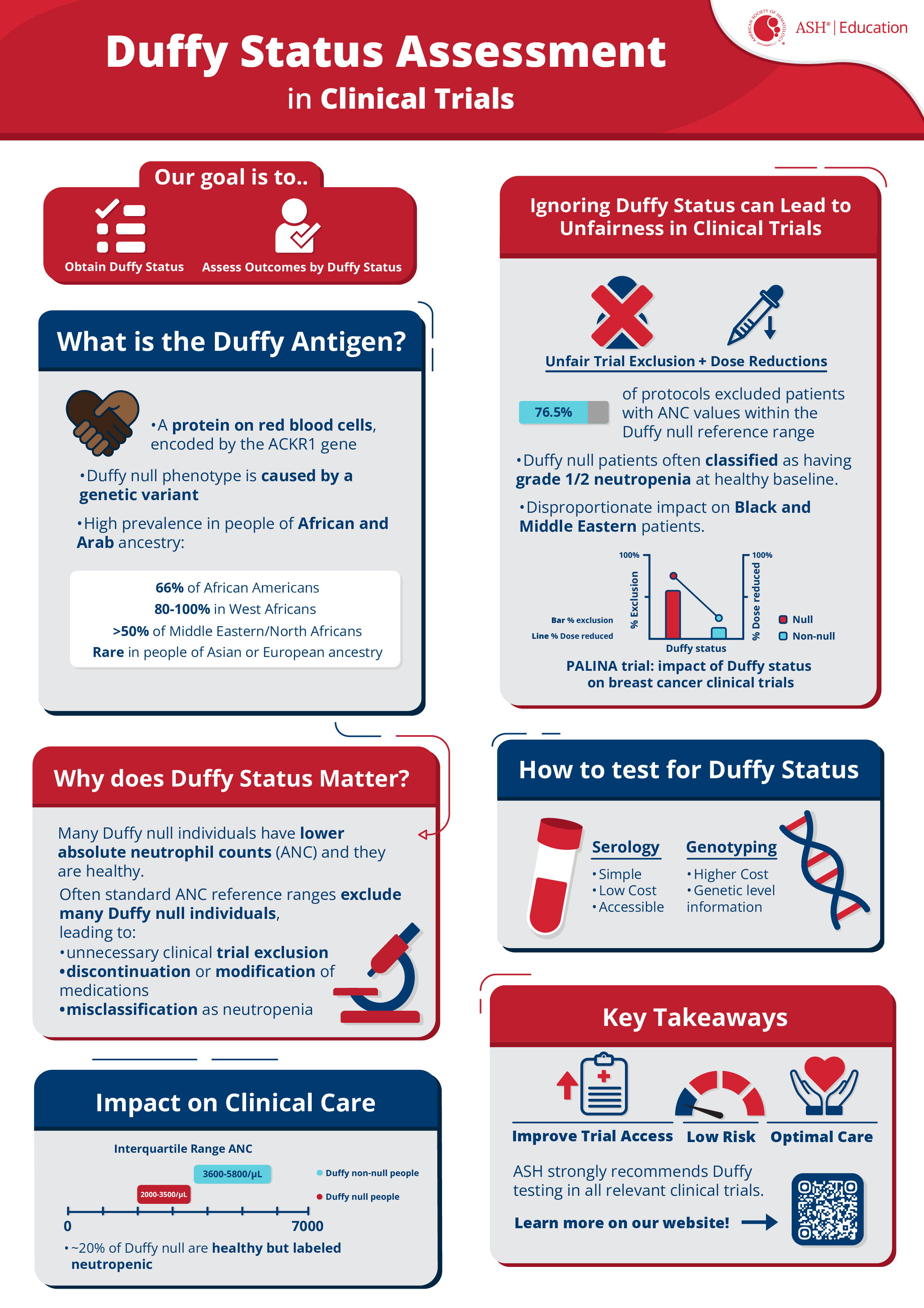
The Duffy blood group system is one of many that are used to classify blood types. People with the Duffy-null blood type often have a lower absolute neutrophil count (ANC) than most other people. This is called Duffy-null associated neutrophil count (DANC).
Individuals with the Duffy-null phenotype have no increased risk of infection but are often incorrectly labeled as having neutropenia. This can result in unnecessary, expensive, and invasive testing, delayed or discontinued chemotherapy or other critical medications, exclusion from clinical trials, and other negative consequences.
Through a multifaceted approach, ASH aims to improve the quality of care for individuals with DANC.
Clinical Recommendations
Many individuals with the Duffy null variant have lower absolute neutrophil counts (ANC) at baseline without increased infection risk. This may have significant implications for trial eligibility, medication dosing, and even health outcomes in clinical trials. ASH strongly recommends integrating Duffy testing into all relevant clinical trials to generate data to ensure optimal eligibility criteria and dose-modification criteria, assess outcomes by Duffy status, and allow for personalized patient care. This section outlines key considerations and emerging recommendations for integrating Duffy status assessment into clinical research.


Educational Resources
This educational program aims to improve awareness and understanding of Duffy-null associated neutrophil count (DANC), a common and under-recognized source of health inequality worldwide. Through patient case studies, the program will explain how to distinguish DANC from pathological neutropenia and guide learners through its genetic basis and possible mechanisms. The program will also review the challenges that people with DANC may encounter and how to mitigate them. View the full course on ASH Academy On Demand or access the individual resources below.
DANC Diagnosis: Printable Resources

Neutropenia Navigator: An Approach to Interpret Absolute Neutrophil Count (ANC)
It’s not always easy to tell when low Associated neutrophil count (ANC) is something to worry about. This handy practical guide to the hierarchy of concern for low ANC is great to print and keep in your practice. Download the Algorithm

A Guide to Duffy-null Associated Neutrophil Count (DANC): Provider-Patient Consultation Tool
Duffy-null associated neutrophil count (DANC) is often not fully understood, leading to unnecessary medical tests and health inequalities. This consultation tool serves as a practice aid to helps patients learn more about DANC, the challenges it may present, and steps they can take to ensure their health needs are met. Share it to support your patients in navigating their healthcare journey. Download the Consultation ToolDANC Diagnosis: Interactive Learning
Understanding Duffy Status and Neutrophil Count: An Interactive Approach eModule
What connects the Duffy blood group to widespread health inequalities? In the first of an upcoming three-module course, test your diagnostic skills with six case studies, learn more about Duffy-null associated neutrophil count and what it means for your patients. Go to the eModule

{kind=link}
Mechanisms and Epidemiology of DANC

Mechanisms and Epidemiology of Duffy-null Associated Neutrophil Count (DANC) eModule
What lies behind Duffy-null associated neutrophil count (DANC) and how can we discuss it with our patients? Follow a conversation with a patient to review our knowledge of the epidemiology and biological basis of DANC, and how it affects healthcare in this interactive e-module. Go to the eModuleAbsolute Neutrophil Count (ANC) by Duffy Status Project
ASH is at the forefront of addressing a critical health equity concern through its groundbreaking initiative - the Reconsideration of Absolute neutrophil count (ANC) Reference Ranges by Duffy Status. The initiative is funded by a grant from the Doris Duke Foundation and seeks to ensure that all individuals, especially those with Duffy-null associated neutrophil count (DANC), receive optimal care by redefining ANC reference ranges based on Duffy status.
Absolute Neutrophil Count by Duffy Status Among Healthy Black and African American Adults
Approximately two of three people identifying as Black in the U.S. are expected to have the Duffy-null phenotype. Of note, race and ethnicity are not biological facts but sociopolitical constructs. Genetic traits do not obey racial boundaries or geographic constructs, so using them as proxies requires extreme caution. While the Duffy-null phenotype is not exclusive to African or Arabian Peninsula genetic ancestry, it is most commonly found among these populations.
Additional Resources
Key Publications
- When non-Whiteness Becomes a Condition
- Absolute Neutrophil Count by Duffy Status Among Healthy Black and African American Adults
- Race, Genotype, and Azathioprine Discontinuation: A Cohort Study
- Development of Duffy Null–Specific Absolute Neutrophil Count Reference Ranges
- The Duffy Null Phenotype — Addressing a Source of Discrimination in Cancer Care
Additional Publications and Resources
- 2022 ASCP Choosing Wisely Recommendation includes Duffy-null testing
- Invisible Infrastructure in Haematology: Neutrophil Reference Ranges and the Duffy-null Phenotype
- The Duffy-null genotype and risk of infection
- Duffy null genotype or Fy(a-b-) phenotype are more accurate than self-declared race for diagnosing benign ethnic neutropenia in Brazilian population
- Ethnic neutropenia and treatment delay in African American women undergoing chemotherapy for early-stage breast cancer
- Neutrophil Counts in Healthy South African Infants: Implications for Enrollment and Adverse Event Grading in Clinical Trials in an African Setting
- The DARC Side of Inflamm-Aging: Duffy Antigen Receptor for Chemokines (DARC/ACKR1) as a Potential Biomarker of Aging, Immunosenescence, and Breast Oncogenesis among High-Risk Subpopulations
- Atypical chemokine receptor 1 on nucleated erythroid cells regulates hematopoiesis: https://pubmed.ncbi.nlm.nih.gov/28553950/
- The American Society for Clinical Pathology Expands List of Commonly Used Tests Physicians and Patients Should Question in Collaboration with ASCLS and ASM
Presentations
- What is a “Normal” Neutrophil Count? The Duffy Red Cell Antigen, Ancestry, Genetics and Evolution
- “Where Have All the Neutrophils Gone?”
Terms and Definitions
Questions
If you have questions or require additional information regarding DANC or the ANC by Duffy Status project, please contact [email protected].